Before you accept your treatment modality, you should know about various surgical options available to treat your arthritic knee.
Various surgical options, in short, are as follows:
High Tibial Osteotomy:
It is a procedure to correct the inward angulation of the leg. This is only useful in the younger age group (in the ’40s) before arthritis has set in. Once joint degeneration has occurred, this surgery has a very limited role
Arthroscopy
It is endoscopic and stitchless surgery. You need half a day of admission to the hospital. You will be allowed to perform routine activities from day one of the surgery. Arthroscopy has a palliative role in Osteoarthritis rather than a curative one. It can improve the locking of the joint and it does help in acute exacerbation of pain because of a degenerative meniscal tear. In some cases of early arthritis, it works wonderfully well for a few years.

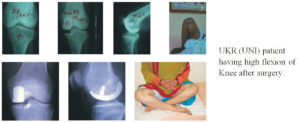
Unicondylar Knee Arthroplasty:
This surgery is indicated in patients who have moderate to severe degrees of pain but the degeneration of the joints is limited only to one part of the joint and the joint is stable with intact ligaments. It is not suitable for obese/overweight patients. This surgery is wonderfully accepted by patients because it requires a smaller skin cut, provides quick recovery and a full range of movements to the knee. You can even sit on the floor and perform religious activities without any trouble.
Total Knee Arthroplasty:
When the knee is severely damaged by arthritis or injury, it may be hard for you to perform simple activities such as walking or climbing stairs. You may even begin to feel the pain while you are sitting or lying down. In such a condition, you may want to consider total knee replacement surgery, which is considered as the best pain-relieving medicine with reliable results.
Knee replacement was first performed in 1968, improvement in surgical materials and techniques since then has greatly increased its effectiveness. About 2,67000 total knee replacements are performed each year in the United States alone and a much larger number in the world as a whole. Joint Replacement is a very successful procedure in orthopedic surgery today. In fact unlike the hip replacement where the head and neck of the femur are replaced by the artificial parts, in the knee the surgery involves only resurfacing of the worn-out cartilage, exactly the wayworn out tooth is resurfaced by the dentist using a cap fixing it with cement. The present-day results have become so sure and smooth that undergoing the surgery has become an easy task. Knee Replacement (Total or partial) does have a definitive and almost a complication-free outcome in skilled hands.
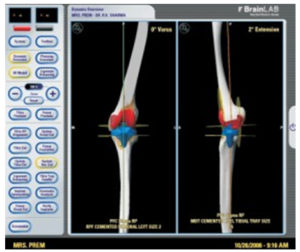
Recent Advances In Total Knee Arthroplasty:
The major recent developments in the world today are, the use of Mobile bearing Knee Implants (because of their documented longer survival rate), minimally invasive surgery, computer-assisted surgery, use of high flexion designs, which provide near full movements to the knee, Patient matched Implants and Instrumentation, Newer materials and methodology in the manufacturing of the Implants for better survivability like X3 Poly.
The Mobile Bearing Knee designs have documented longer survival (LCS design has a documented survival up to 20-25 years). This longer survival of mobile-bearing joint designs is because of its better design and relative mobility between the components, and larger contact area (1400 sq mm) as compared to Fixed Bearing implants (200 sq mm). This is the most suitable implant for relatively younger and active or obese patients.
These days we are doing knee replacement with just 4” incision (minimally invasive surgery) in suitable persons.
The survivability of Implant depends on the materials used. With ever-improving material science, we can now say that the implants will be long-lasting. One newer advancement is the use of Second Generation Highly Cross-linked Polyethylene or X3 Poly which has an extremely small wear quotient and longer life.
Patient matched Implants or Instrumentation is a newer Innovation in TKR. In this, a model of patient’s knee is made with the help of a CT scan or MRI. Then based on that, Instruments are made which are customized according to the specific requirements of the patient. This increases the accuracy of the surgery.
One is allowed to go to the bathroom on the second day of the surgery, exercises on the bed are started on the day of surgery. One needs to use walker or elbow sticks for about 2 to 3 weeks. Usually, in 3 to 4 weeks you may start performing normal routine activities like driving a car, going to market, etc.
Recovery depends upon the quality of surgery done, determination of the patient and inputs of the surgeon. Usually, in our patients, the movement of 00 to 1200-1400 is achieved after surgery.
The age at which you should opt for surgery is not relevant. Surgery is an option when you have a significant problem and your surgeon confirms the same. There is no substance in the suggestion that one should carry on suffering as long as one can and then go for surgery when the suffering is unbearable when options (mobile-bearing high flexion knee) with a life span of 20-25 years are available. Youngest patients operated by me are 23 years old and the oldest is 92 years. Obesity also is not an obstacle; Patients up to the weight of 147 Kgs have been successfully treated under my care.
The decision for whether one should opt for this surgery, should be a co-opted one between you, your family and your surgeon. You should weigh the benefits of the surgery with respect to the problems you are facing.